
Two things common between aviation and anesthesia is to get everyone high and to ensure a safe experience. Patient safety, as defined by WHO, is the reduction of risk of unnecessary harm associated with healthcare to an acceptable minimum8. Here, “harm” is the range of undesirable outcomes and “unnecessary” implies that this harm was preventable2. Most of these errors are iatrogenic in origin caused by accident or neglect.
A prospective study in 2008 found that risk of death under anesthesia increased four to five times when basic monitoring (like checking pulse) was not provided for anesthetized veterinary patients, amongst whom many deaths were reported in healthy animals, which could have been prevented by basic monitoring techniques1. Safety incidents like extravasation of drugs through failed IV cannula placement, medication error, not performing machine leak check, closed pop-off valve, oesophageal intubation and equipment failure are known to occur in many practices.
In a 3-year long analysis, Wallis et al. reported safety incidents occurred in 0.4-0.8% of hospital visits, which does not seem like a significant number, but amongst these incidents more than half the incidents were medication errors. These patients either received wrong drug, wrong labelling of drug in syringe, wrong dose, drug was administered by the wrong route, and DRUG ADMINSITERED TO THE WRONG PATIENT! Communication errors with clients like misinformation, illegible handwriting on anesthesia logs or incorrectly interpreted information by other doctors formed 30% of the cause of safety incidents10.

Why things go wrong?
Anesthetic drugs are rapidly acting with significant physiological effects (CNS and cardiorespiratory depression) and very narrow margin of error. Performing surgical procedures under a vulnerable physiological state using electronic monitoring systems is very dynamic and unpredictable. It would be simple to assume that people are the problem and need to be fixed. Human errors cannot be eliminated in such situations4. People perform tasks and take decisions to the best of their abilities. These actions are highly influenced and systematically linked to the initial training, workplace, colleagues, guidance from seniors, tools and work environment7.
Black box
Since we have identified errors, it’s time to find their source. Learning culture should be encouraged by reporting the errors made, instead of playing a blame- game. Safety incident reporting involves discussing errors, analyzing them and improving the outcomes. It should be investigated as “Who” was involved, “What” happened, “When”, “Where”, “Why” and “How” it happened7.
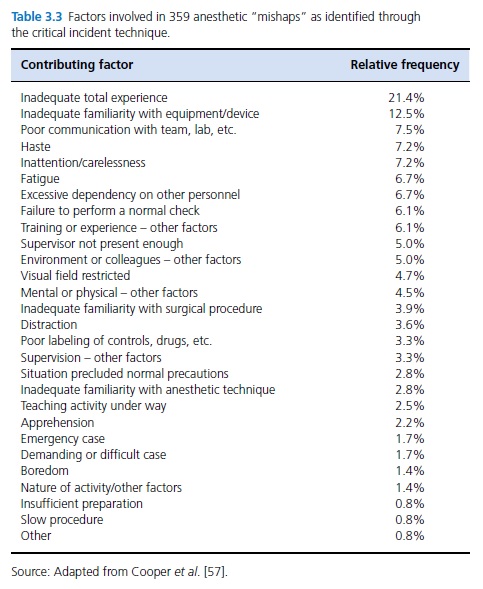
In 1978, 359 safety incidents were investigated out of which found 82% were attributed to human error. Many of these incidents were found to be made by residents under training, and could be averted by a more structured approach by appropriately mentoring residents3.
Problem solving mode on!
In order to reduce errors, improve performance and ensure patient safety, a tangible and effective tool is a “Checklist”. Checklists are an organized list of actions or criteria that can be recorded as present/absent; when each item is considered or complete5. It ensures acceptable safety practices and encourages communication amongst team members.
Each activity while performing anesthesia can be divided into sections, and each section subdivided into specific actions. Begin with admitting a patient for surgery:
- Confirm fasting status.
- Perform physical exam.
- Client communication about the procedure and anesthesia risks.
- Explain and sign consent form.
- Assign assistants for the surgery patient.
This is a simple example of how activities are divided into actionable steps. Anesthesia checklists comprise of 3 major sections: “Sign in”- Before induction of anesthesia, “Time out”- Before skin incision, and “Sign out”- Before patient leaves the OR11. These sections should have specific tasks customized for the clinic/hospital and suitable to its functioning. Language used should easily be understood by all members of the surgical team. Here is an example from RCVS Knowledge16:
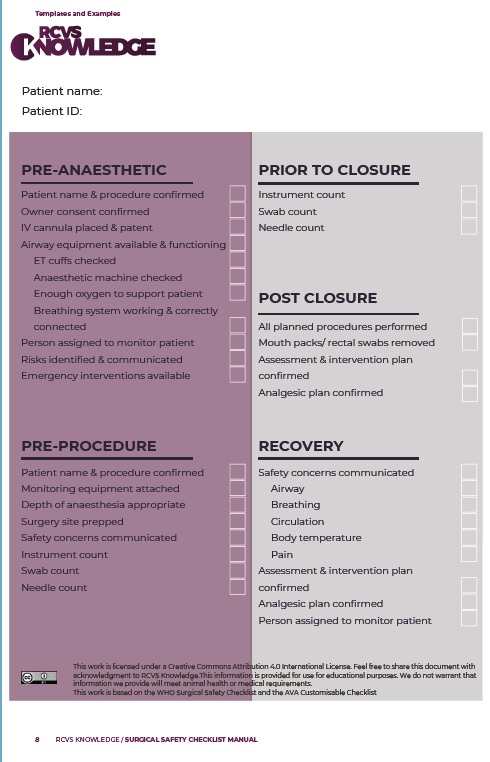
In a practice, safety incidences like unintentional closed pop- off valve and oesophageal intubation were noted to occur frequently. A checklist designed for the clinic included checks for these two incidents. The frequency of these incidents dropped by 75% in a year and more positive patient outcomes were reported6. A recent study investigated 8000 surgical procedures before and after introducing checklists and presurgical briefing amongst surgery team reduced mortality, unplanned and revision surgeries and lesser postoperative hospital stay duration9.
Countermeasures, like checklists, which are newly implied in a practice should not be assumed to always work and show improvement. Team members should have adequate time to familiarize themselves to this new activity and make changes wherever necessary. The ultimate aim is to improve team performance and patient outcome with least or no safety incidents.
Edited by Prajakta Alase
Citations:
- Brodbelt, D.C., Blissitt, K.J., Hammond, R.A., Neath, P.J., Young, L.E., Pfeiffer, D.U. and Wood, J.L., 2008. The risk of death: the confidential enquiry into perioperative small animal fatalities. Veterinary anaesthesia and analgesia, 35(5), pp.365-373.
- Catchpole, K., Bell, M.D.D. and Johnson, S., 2008. Safety in anaesthesia: a study of 12 606 reported incidents from the UK National Reporting and Learning System. Anaesthesia, 63(4), pp.340-346.
- Cooper, J.B., Newbower, R.S., Long, C.D. and McPeek, B., 1978. Preventable anesthesia mishaps: a study of human factors. Anesthesiology, 49(6), pp.399-406.
- Donaldson, M.S., Corrigan, J.M. and Kohn, L.T. eds., 2000. To err is human: building a safer health system.
- Hales, B.M. and Pronovost, P.J., 2006. The checklist—a tool for error management and performance improvement. Journal of critical care, 21(3), pp.231-235.
- Hofmeister, E.H., Quandt, J., Braun, C. and Shepard, M., 2014. Development, implementation and impact of simple patient safety interventions in a university teaching hospital. Veterinary anaesthesia and analgesia, 41(3), pp.243-248.
- McMillan, M. and Pang, D.S., 2024. Introduction to Patient Safety. Veterinary Anesthesia and Analgesia: The Sixth Edition of Lumb and Jones, pp.24-39.
- Runciman, W., Hibbert, P., Thomson, R., Van Der Schaaf, T., Sherman, H. and Lewalle, P., 2009. Towards an International Classification for Patient Safety: key concepts and terms. International journal for quality in health care, 21(1), pp.18-26.
- Tschan, F., Keller, S., Semmer, N.K., Timm-Holzer, E., Zimmermann, J., Huber, S.A., Wrann, S., Hübner, M., Banz, V., Prevost, G.A. and Marschall, J., 2022. Effects of structured intraoperative briefings on patient outcomes: multicentre before-and-after study. British Journal of Surgery, 109(1), pp.136-144.
- Wallis, J., Fletcher, D., Bentley, A. and Ludders, J., 2019. Medical errors cause harm in veterinary hospitals. Frontiers in Veterinary Science, 6, p.12.
- World Health Organization (WHO) Surgical Safety Checklist (SSC) – Implementation Manual 2009. https://www.who.int/publications/i/item/9789241598590 (accessed March 2022.)
- https://www.nbcnews.com/health/health-news/when-vets-make-mistakes-pets-pay-price-flna1c9446213
- https://timesofindia.indiatimes.com/spotlight/isb-executive-educations-leadership-with-ai-programme-empowers-leaders-to-transform-operations-through-technology/articleshow/112280654.cms
- https://www.nbcchicago.com/news/local/dog-scheduled-for-teeth-cleaning-was-spayed-by-chicago-vet-instead-owner-says/3515251/
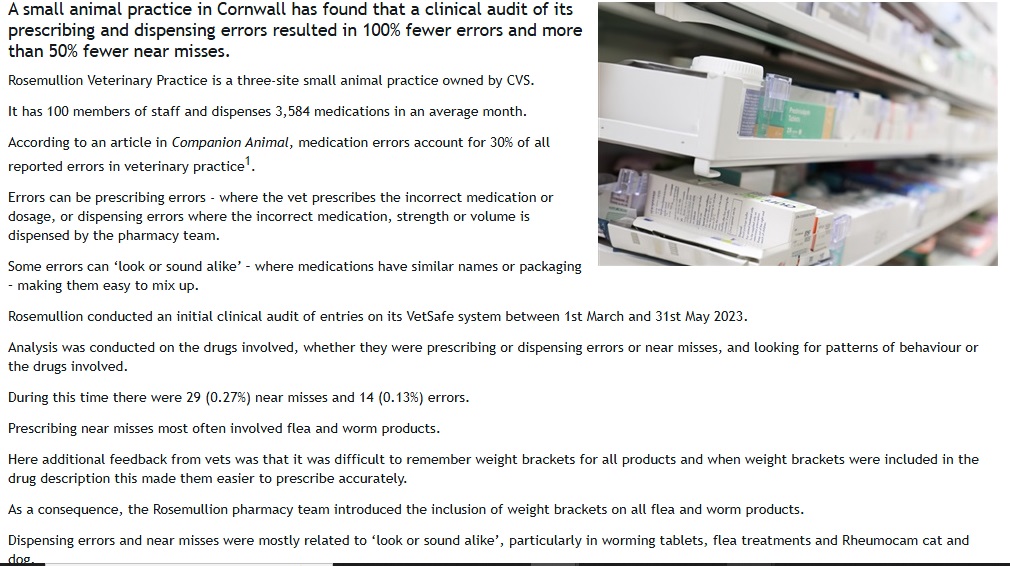
- https://www.vetsurgeon.org/b/veterinary-news/posts/vet-practice-audit-reduces-medication-errors-by-100
- https://knowledge.rcvs.org.uk/document-library/surgical-safety-checklist-manual/




Leave a comment